





Overview
Snoring is the hoarse or harsh sound that occurs when air flows past relaxed tissues in your throat, causing the tissues to vibrate as you breathe. Nearly everyone snores now and then, but for some people it can be a chronic problem. Sometimes it may also indicate a serious health condition. In addition, snoring can be a nuisance to your partner.

Lifestyle changes, such as losing weight, avoiding alcohol close to bedtime or sleeping on your side, can help stop snoring.

In addition, medical devices and surgery are available that may reduce disruptive snoring. However, these aren’t suitable or necessary for everyone who snores.
Symptoms
Snoring is often associated with a sleep disorder called obstructive sleep apnea (OSA). Not all snorers have OSA, but if snoring is accompanied by any of the following symptoms, it may be an indication to see a doctor for further evaluation for OSA:
- Witnessed breathing pauses during sleep
- Excessive daytime sleepiness
- Difficulty concentrating
- Morning headaches
- Sore throat upon awakening
- Restless sleep
- Gasping or choking at night
- High blood pressure
- Chest pain at night
- Your snoring is so loud it’s disrupting your partner’s sleep
- In children, poor attention span, behavioral issues or poor performance in school
OSA often is characterized by loud snoring followed by periods of silence when breathing stops or nearly stops. Eventually, this reduction or pause in breathing may signal you to wake up, and you may awaken with a loud snort or gasping sound.
You may sleep lightly due to disrupted sleep. This pattern of breathing pauses may be repeated many times during the night.
People with obstructive sleep apnea usually experience periods when breathing slows or stops at least five times during every hour of sleep.
When to see a doctor
See your doctor if you have any of the above symptoms. These may indicate your snoring is associated with obstructive sleep apnea (OSA).
If your child snores, ask your pediatrician about it. Children can have OSA, too. Nose and throat problems — such as enlarged tonsils — and obesity often can narrow a child’s airway, which can lead to your child developing OSA.
Causes
Snoring can be caused by a number of factors, such as the anatomy of your mouth and sinuses, alcohol consumption, allergies, a cold, and your weight.
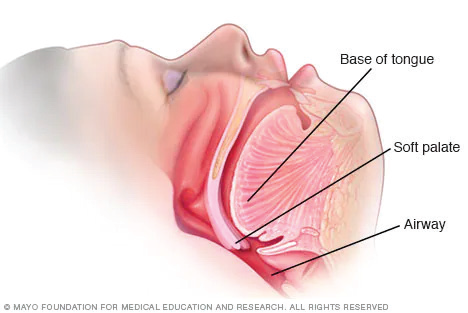
When you doze off and progress from a light sleep to a deep sleep, the muscles in the roof of your mouth (soft palate), tongue and throat relax. The tissues in your throat can relax enough that they partially block your airway and vibrate.
The more narrowed your airway, the more forceful the airflow becomes. This increases tissue vibration, which causes your snoring to grow louder.
The following conditions can affect the airway and cause snoring:
- Your mouth anatomy. Having a low, thick soft palate can narrow your airway. People who are overweight may have extra tissues in the back of their throats that may narrow their airways. Likewise, if the triangular piece of tissue hanging from the soft palate (uvula) is elongated, airflow can be obstructed and vibration increased.
- Alcohol consumption. Snoring can also be brought on by consuming too much alcohol before bedtime. Alcohol relaxes throat muscles and decreases your natural defenses against airway obstruction.
- Nasal problems. Chronic nasal congestion or a crooked partition between your nostrils (deviated nasal septum) may contribute to your snoring.
- Sleep deprivation. Not getting enough sleep can lead to further throat relaxation.
- Sleep position. Snoring is typically most frequent and loudest when sleeping on the back as gravity’s effect on the throat narrows the airway.
Risk factors
Risk factors that may contribute to snoring include:
- Being a man. Men are more likely to snore or have sleep apnea than are women.
- Being overweight. People who are overweight or obese are more likely to snore or have obstructive sleep apnea.
- Having a narrow airway. Some people may have a long soft palate, or large tonsils or adenoids, which can narrow the airway and cause snoring.
- Drinking alcohol. Alcohol relaxes your throat muscles, increasing the risk of snoring.
- Having nasal problems. If you have a structural defect in your airway, such as a deviated septum, or your nose is chronically congested, your risk of snoring is greater.
- Having a family history of snoring or obstructive sleep apnea. Heredity is a potential risk factor for OSA.
Complications
Habitual snoring may be more than just a nuisance. Aside from disrupting a bed partner’s sleep, if snoring is associated with OSA, you may be at risk for other complications, including:
- Daytime sleepiness
- Frequent frustration or anger
- Difficulty concentrating
- A greater risk of high blood pressure, heart conditions and stroke
- An increased risk of behavior problems, such as aggression or learning problems, in children with OSA
- An increased risk of motor vehicle accidents due to lack of sleep










Add Comment